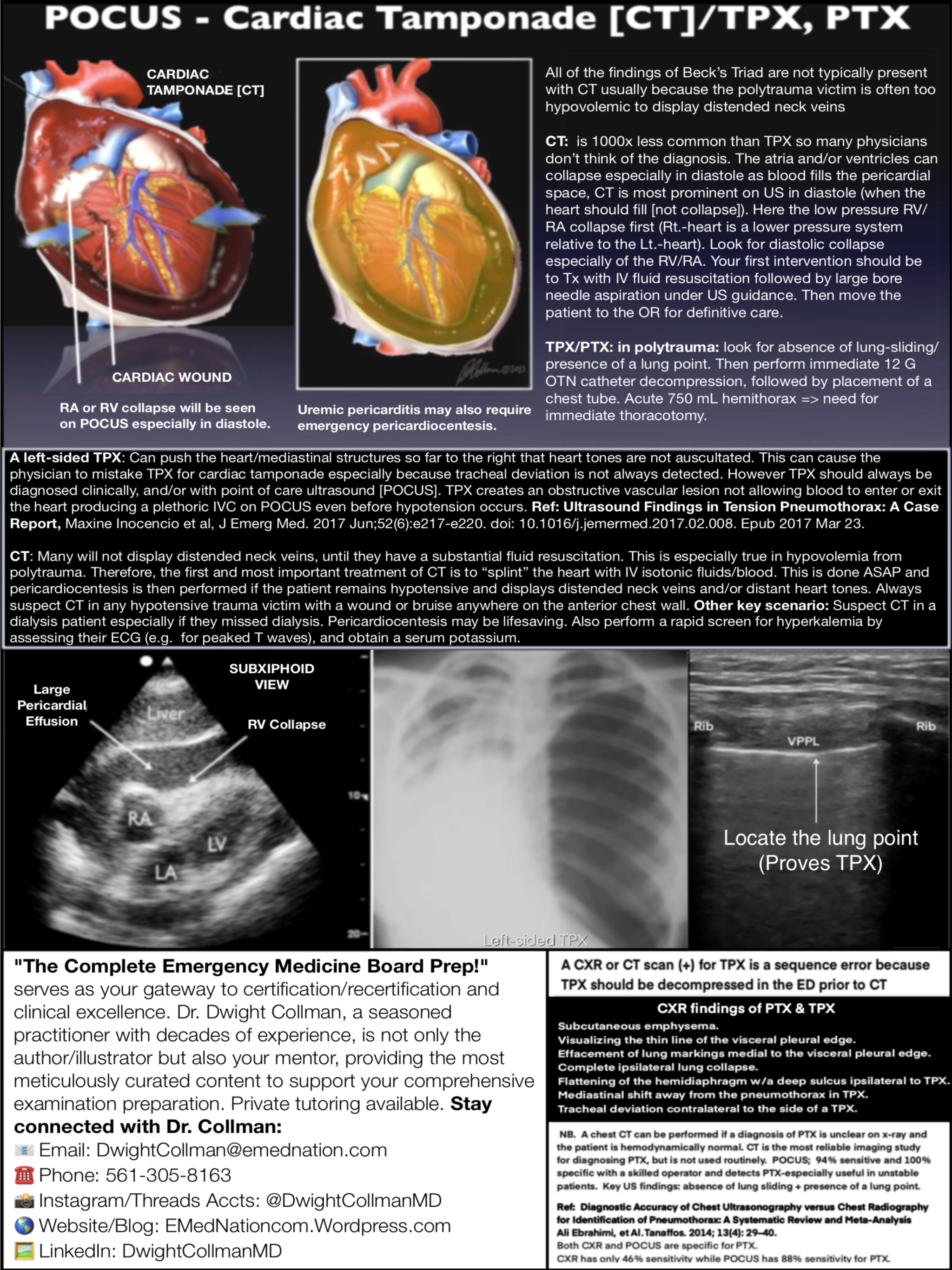
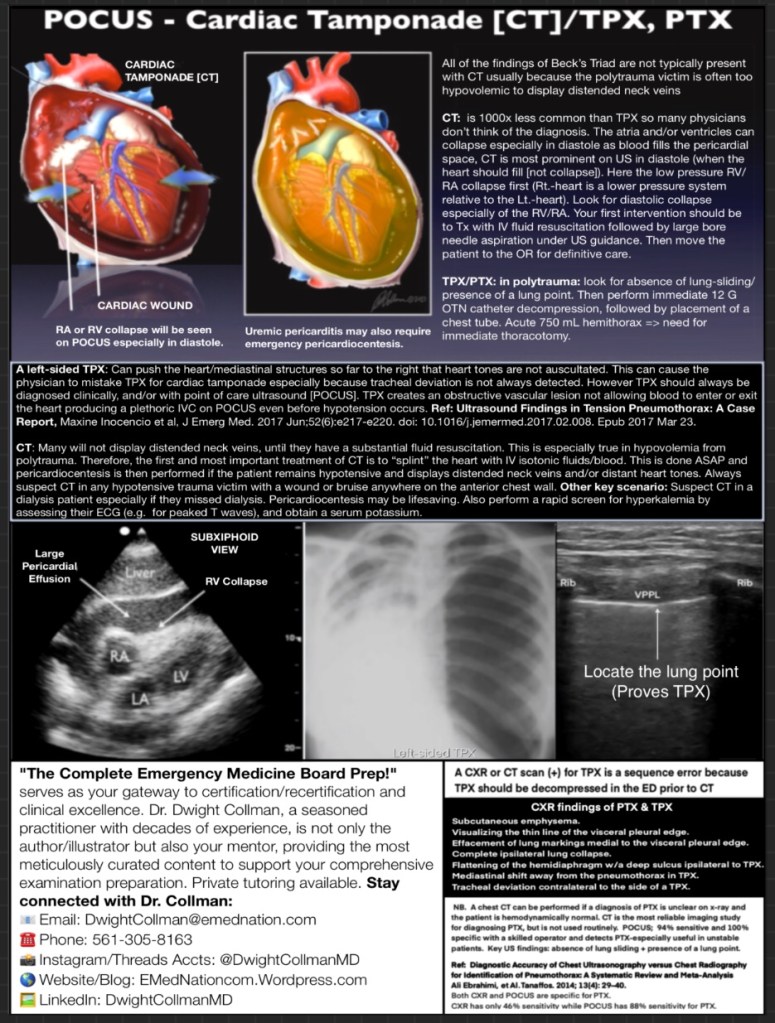
❑❑ Might a left-sided TPX be confused with cardiac tamponade [CT]?
Answer: Yes. A left-sided TPX: Can push the heart/mediastinal structures so far to the right that heart tones are not auscultated over the anatomical cardiac apex. Lack of heart tones and neck vein distention may then cause the physician to favor a presumptive diagnosis of cardiac tamponade especially because tracheal deviation may not be discernible with TPX. Other signs of left TPX should be sought, e.g., inability to ventilate the patient, ipsilateral percussion tympany, and subcutaneous emphysema. TPX should always be diagnosed clinically, and/or with point of care ultrasound [POCUS]. TPX creates an obstructive vascular lesion not allowing blood to enter or exit the heart producing a plethoric IVC which can be visualized on POCUS even before hypotension occurs. Ref: Ultrasound Findings in Tension Pneumothorax: A Case Report, Maxine Inocencio et al, J Emerg Med. 2017 Jun;52(6):e217-e220. doi: 10.1016/j.jemermed.2017.02.008. Epub 2017 Mar 23. 29-40.
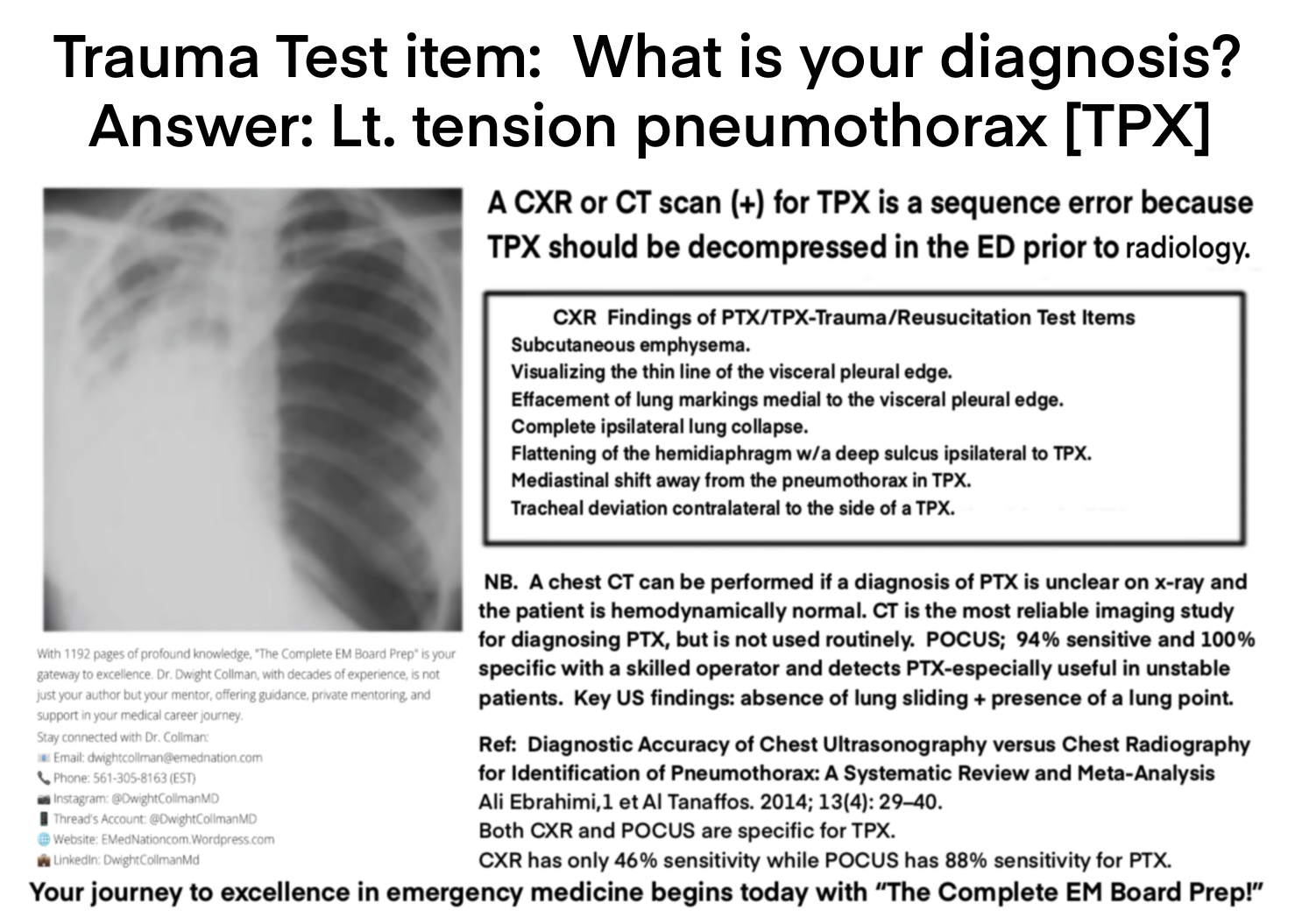
❑❑ How does the diagnostic accuracy of chest ultrasonography [CUS] compare with supine chest x-ray [CXR] in the detection of a pneumothorax [PTX]?
Answer: Both are specific; however, plain supine CXR had a sensitivity of only 46% while CUS had a sensitivity of 88%. This was found in a 2014 meta-analysis: CUS was superior to CXR even after adjusting for possible sources of heterogeneity. Ref: Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax. A Systematic Review and Meta-Analysis. Ali Ebrahimi et Al. Tanaflos 2014; 13(4) 29-40.
❑❑ What are the plain radiographic (CXR) findings of PTX and TPX?
Answer: 1. Subcutaneous emphysema; 2. Visualizing the thin line of the visceral pleural edge; 3. Effacement of lung markings medial to the visceral pleural edge; 4. Complete ipsilateral lung collapse; 5. Flattening of the hemidiaphragm with a deep sulcus ipsilateral to a TPX; 6. Mediastinal shift away from the pneumothorax in TPX; 7. Tracheal deviation contralateral to the side of a TPX.
Your journey to board certification and excellence in emergency medicine begins today with “The Complete EM Board Prep”!
The Complete EM Board Prep!
1192 page training program for emergency physicians preparing for board certification.
$899.00
Sample of complimentary periodic updated content.
Promotional fee for residents-in-training $499.00 US
The Complete Emergency Medicine Board Prep!
Discount for residents in training. Please email a copy of a letter of verification from your residency program to DwightCollman@emednation.com. The complete preparation you need to prepare for certification in emergency medicine. 1192 pages. Written and illustrated by Dwight Collman, MD. This text is now available as of Nov 1, 2023.
📘 **”The Complete EM Board Prep” – Elevate Your Emergency Medicine Expertise in 2023!**
Embark on a transformative journey to excellence with “The Complete EM Board Prep,” a meticulously curated 1192-page masterpiece by Dr. Dwight Collman, MD. Fully updated in 2023, this comprehensive guide is your passport to success in board certification preparation and excelling in your clinical practice of emergency medicine.
🌟 **A Legacy of Expertise**
Since its inception in 1989 with the groundbreaking “Oral Board Tutorial!” program, this resource has evolved into a comprehensive offering that now includes the transformative 8-Day Interactive Review. With an impressive attendance of over 12,000 esteemed colleagues, these programs are synonymous with excellence in emergency medicine education. Dr. Collman, a seasoned practitioner with over four decades of invaluable experience, seamlessly integrates profound study advice and methodology into meticulously crafted clinical test items, specially curated for qualifying, oral, and ConCert™ examinations.
🔍 **Precision meets Comprehensiveness**
Dr. Collman’s mission is clear – to strike a perfect balance between comprehensive content and laser-focused study materials. In the ever-evolving medical landscape, this text evolved in tandem, ensuring its relevance extends beyond board certification, catering to all practicing emergency medicine physicians. Dr Collman also regularly provides updated content in his blog.
📚 **A Wealth of Knowledge at Your Fingertips**
Immerse yourself in a quick-reading format that unveils pearls of wisdom across several chapters of study advice, thousands of rapid-reading test items, detailed clinical test items, a comprehensive guide to approaching the oral examination, detailed oral exam case simulations, including relevant pathophysiology questions and examiner notes, dozens of carefully crafted/curated pictorial items, and Dr. Collman’s key outlines extracted from the Study Guide. Dr. Collman’s dedication to creating medical illustrations enhances your grasp of complex pathophysiology. Plus, with “The Complete EM Board Prep,” rest assured you won’t need any other board prep program or materials – everything you need is within these comprehensive pages.
🗺️ **Your Path to Excellence – Divided into Seven Sections**
Section I serves as an essential introduction, guiding you through the intricate process of acquiring, retaining, and skillfully applying your knowledge on these examinations – how to apply your fundamental knowledge of patient care and test-taking.
Section II encompasses thousands of rapid test items meticulously categorized into various medical content areas, empowering you to excel in qualifying and ConCert board examinations.
Section III is a dedicated space for comprehensive ConCert exam preparation, presenting clinically oriented sample questions in intricate detail.
Section IV – the Oral Board Tutorial – demystifies the examination process, an extensive and comprehensive approach to all cases, offering insights into performance ratings and scoring criteria. Dr. Collman’s detailed candidate and examiner instructions guide you to maximize your case scores. This is the completely updated version of his 5-day live program.
Section V comprises 27 detailed board-level case simulations, equipped with examiner notes, insights, and pathophysiology, closely simulating the actual examination content. Every examination detail and pitfall is presented. Remember, Dr. Collman has been a test item writer for two recognized emergency medicine boards, and he also trained oral examiners for many years.
Section VI introduces pictorial test items that parallel the critical visual stimuli in all ABEM examinations – these have been proven to accurately represent the examinations.
Section VII includes Dr. Collman’s personal outlines, highlighting essential keywords, principles, and updated information.
With 1192 pages of profound knowledge, “The Complete EM Board Prep” is your gateway to excellence. Dr. Dwight Collman, not just your author but your mentor, offers guidance, private tutoring, and support in your medical career journey. He regularly provides additional content on his blog, so definitely follow him there too. Physicians-in-training currently receive a substantial promotional discount. This material will serve you well throughout your career.
🌐 Order Now and Stay Updated!
Visit his website and blog: EMedNationcom.Wordpress.com
📲 **Follow Dr. Collman’s Blog for Updates and Insights:**
📧 Email: dwightcollman@emednation.com
📞 Phone: 561-305-8163 (EST)
📷 Instagram: @DwightCollmanMD
📱 Thread’s Account: @DwightCollmanMD
💼 LinkedIn: DwightCollmanMD
Your journey to excellence in emergency medicine begins today with “The Complete EM Board Prep”!
Your journey to board certification and excellence in emergency medicine begins today with “The Complete EM Board Prep”!
The Complete EM Board Prep!
1192 page training program for emergency physicians preparing for board certification.
$899.00
Promotional fee for residents-in-training $499.00 US
The Complete Emergency Medicine Board Prep!
Discount for residents in training. Please email a copy of a letter of verification from your residency program to DwightCollman@emednation.com. The complete preparation you need to prepare for certification in emergency medicine. 1192 pages. Written and illustrated by Dwight Collman, MD. This text is now available as of Nov 1, 2023.
❑❑What is the purpose of the NEXUS criteria & Canadian C-Spine Rule [CCR]? How do these 2 rules compare when IDing low risk pts for C-spine injuries [CSI] in blunt trauma? How do you perform each rule?
Answers: Both rules are clinical decision rules that can help physicians determine which trauma pts require C-spine imaging. Both rules can ID low risk pts & reduce imaging, but CCR showed superior overall performance compared to NEXUS (CCR appears to have higher S/S overall based on a recent meta-analysis comparing the 2 rules). Both rules should be used to try to reduce unnec. imaging, but imaging should not be withheld in higher risk pts. NB. Proper clinical judgment is still required in applying and interpreting these 2 rules.
How to Perform the Rules:
NEXUS criteria: consist of 5 low risk criteria. If any are met, imaging can be avoided:
– No midline cervical tenderness.
– No focal neurological deficit
– Normal alertness
– No intoxication
– No painful distracting injury
The CCRcriteria: consist of 3 high risk factors & 5 low risk factors. Imaging is indicated if any high risk factors are present. Imaging can potentially be avoided if all low risk factors are met:
3 High risk factors (image if any present):
– Age ≥ 65 yrs.
– Dangerous MOI.
– Paresthesias in extrems.
5 Low risk factors (can consider clearing C-spine if all present):
– Simple rear-end collision.
– Ambulatory at any time.
– Delayed onset of neck pain.
– Absence of midline C-spine tenderness.
– No focal neuro. deficit.
The recent meta-analysis comparing the 2 rules: ref: Baratloo A, Ahmadzadeh K, Forouzanfar MM, Yousefifard M, Farhang Ranjbar M, Hashemi B, Aghili SH. NEXUS vs. Canadian C-Spine Rule (CCR) in Predicting Cervical Spine Injuries; a Systematic Review and Meta-analysis. Archives of Academic Emergency Medicine. 2023;11(1):e66.:
• This meta-analysis Included 35 studies on NEXUS (70,000 pts) & 33 on CCR (33,000 pts).
• “For any CSI, NEXUS had a sensitivity of 0.94 (95% CI 0.88-0.98) and CCR had a sensitivity of 1.00 (95% CI 0.98-1.00). For clinically important CSI, NEXUS had a sensitivity of 0.95 (95% CI 0.89-0.98) and CCR had a sensitivity of 1.00 (95% CI 0.95-1.00).”
• “For any CSI, the AUC was 0.85 for NEXUS and 0.97 for CCR. For clinically important CSI, the AUC was 0.78 (95% CI 0.74-0.81) for NEXUS and 0.94 (95% CI 0.91-0.96) for CCR.”
The 2 original ref. articles:
Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001;286(15):1841-1848.
Hoffman JR, Mower WR, Wolfson AB, Todd KH, Zucker MI. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N Engl J Med. 2000;343(2):94-99.
The Emergency Medicine Oral Examination is a controversial topic: I want to start a dialogue on this particular topic. I have studied this issue for decades. Some will disagree with me because they will say I have a financial incentive to see this process continue. I’m going to start with a basic position…my commentary below. I’m hoping every proponent or opponent physician will join in and comment on this issue. I’m hoping if you have been a candidate or examiner you will join in. Here we go—in simple terms: I stand with ABEM…let me explain:
In the ever-evolving landscape of emergency medicine, the need for rigorous and reliable assessment tools to gauge the competence of our healthcare professionals remains paramount. The American Board of Emergency Medicine (ABEM) Oral Certification Examination stands as a testament to this commitment, serving as a comprehensive evaluation of emergency medicine knowledge, skills, and judgment. While artificial intelligence (AI) has made remarkable strides in recent years, its capabilities still fall short of replicating the intricate cognitive abilities, empathy, and adaptability demanded by the Oral Exam, highlighting the irreplaceable role of human examiners in this critical process.
The ABEM Oral Certification Examination: A Multifaceted Assessment
The ABEM Oral Certification Examination employs a meticulously designed scoring system that delves into eight key performance ratings: Data Acquisition, Problem-Solving, Patient Management, Resource Utilization, Healthcare Provided, Interpersonal Relations and Communication Skills, Comprehension of Pathophysiology, and Professionalism (overall clinical competence). These ratings are further evaluated based on critical actions, inappropriate actions, and even dangerous actions—specific behaviors that distinguish acceptable or unacceptable performance.
This comprehensive evaluation extends beyond the mere assessment of medical knowledge and technical skills. It encompasses the ability to gather information effectively, formulate sound clinical judgments under pressure, communicate clearly and empathetically with patients and colleagues, and adapt to the dynamic and unpredictable nature of emergency medicine settings.
The Limitations of AI in Assessing Human Expertise
While AI can assess the presence or absence of specific actions, it cannot adequately interpret the nuances of candidate language skills, bedside manner, adaptability, and their impact on the overall assessment. Human examiners, on the other hand, are adept at discerning subtle variations in communication, recognizing when a candidate’s statements or responses may indicate underlying gaps in knowledge, reasoning, or empathy.
Human examiners can also assess a candidate’s ability to adapt to dynamic and unpredictable emergency medicine settings, where split-second decisions often hinge on incomplete or ambiguous information. AI, with its current limitations in understanding real-world context and adapting to unpredictable scenarios, cannot adequately assess this crucial aspect of emergency medicine practice.
The Human Touch: Simulating Real-World Patient Encounters
Furthermore, human examiners can interact with candidates in a way that simulates real-world patient encounters, providing specific data as simulated patients, nurses, paramedics, consultants, or admitting physicians. This allows examiners to assess a candidate’s ability to communicate effectively with patients, families, and healthcare colleagues, as well as their ability to gather information, formulate diagnoses, and make sound treatment plans under pressure.
Addressing the Intimidation Factor
The perception that the ABEM Oral Certification Examination is intimidating often stems from self-imposed anxiety rather than the examiner’s demeanor. ABEM examiners undergo rigorous training and are carefully instructed to maintain a fair, objective, and empathetic approach throughout the evaluation process. Their interactions with candidates are designed to elicit the necessary information to assess their competence, not to create an intimidating atmosphere.
In fact, a simulated human, an AI, could easily be just as intimidating to candidates if not more so. Remember, perception is reality. A polygraph test, for example, often elicits physiological responses not because of the human administering the questions but because of the examinee’s perception of the machine’s intrusive ability to detect truth vs. lies. Yet, a polygraph machine doesn’t interact with speech or make scenario adjustments. It is silent. Furthermore, scientific and governmental assessments of polygraphy generally indicate that it is highly inaccurate, susceptible to deception-mitigating countermeasures, and an unreliable means of truthfulness evaluation. Now ABEM is not primarily assessing for deception, although I have experienced some of this in oral examination simulations: physicians sometimes talk just to talk when they lack specific knowledge, e.g. as a response to a pathophysiology question. A human examiner can definitely perceive this and it is why I teach candidates to simply be honest. This would be yet another challenge for an AI.
Empathy and Understanding
Examiners are trained to recognize signs of stress and anxiety in candidates. They can tell when a candidate is having difficulty thinking clearly or expressing themselves effectively. In these cases, examiners will often give the candidate a moment to collect their thoughts or provide them with additional support.
Recognizing and Addressing Unnecessary Self-Deprecation
Examiners can also recognize when a candidate is being unnecessarily self-deprecating. This can sometimes be a sign of anxiety or low self-esteem. In these cases, examiners do try to redirect the candidate’s focus to allow them to maximize their score.
The Importance of Human Judgment
The ability to recognize and respond to these human factors is one of the reasons why human examiners are still essential for the ABEM Oral Certification Examination. AI is not yet able to replicate this level of empathy and understanding.
Safeguarding Fairness and Transparency
Moreover, ABEM employs verifying physicians to monitor the examination process, ensuring that examiners adhere to established guidelines and maintain a professional and respectful environment. This additional layer of oversight further highlights ABEM’s commitment to fairness, transparency, and a focus on patient safety.
Furthermore, examiners disqualify themselves from testing any candidate they know in advance, eliminating any potential for bias or conflict of interest.
The Future of AI in Medical Assessment
The question of how AI would be implemented in the Oral Exam process raises significant concerns about its effectiveness and appropriateness. A machine that spits out images of rhythm strips and radiographs would currently fail to assess the candidate’s ability to interpret and communicate their findings effectively with patients and colleagues. Even if AI were given a human appearance, it would lack the ability to empathize with candidates, understand their concerns and objectives, and make sound clinical assessment decisions based on incomplete or ambiguous information.
In conclusion, the ABEM Oral Certification Examination serves as an indispensable tool for ensuring the competence of emergency physicians, safeguarding patient well-being. While AI holds immense promise for the future, its limitations in replicating human cognitive abilities, empathy, adaptability, and communication skills render it unsuitable for administering the Oral Exam in 2023. Until AI can bridge the chasm between data processing and human expertise as a physician examiner, the irreplaceable role of human examiners in this critical assessment will remain paramount. Now I’m not saying that AI could not eventually simulate a physician as an examiner…just not today.
I hope to hear from the emergency medicine community. Pro or con it doesn’t matter. I’m interested in hearing from everybody. Be well.