The most focused and rigorous prep for ABEM Part I/II/ConCert Exams +AOBEM Exams +BCEM Exams
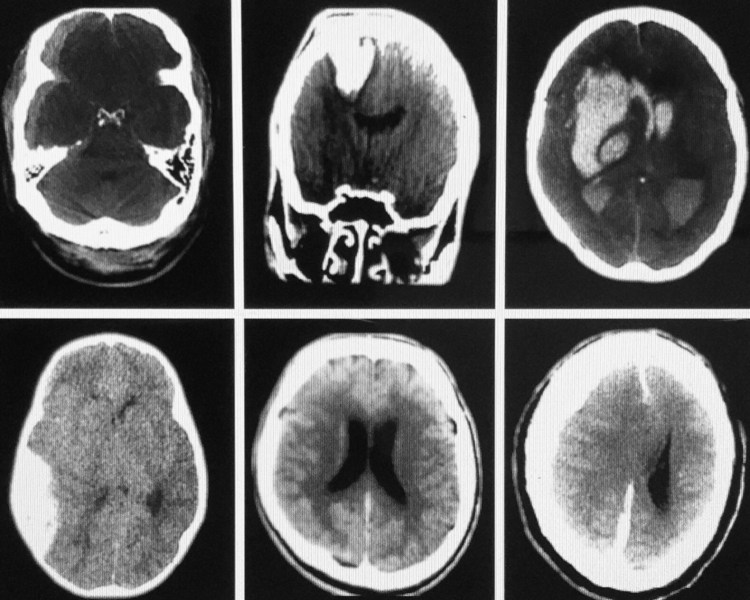
What is the diagnosis in each of these six patients? Assume they all arrive at the same time, i.e., this is a mass casualty event – How would you prioritize the overall management and transfer of any of these patients to a neurosurgeon?
Discussion: note: (On exams some images are field test items [not scored].
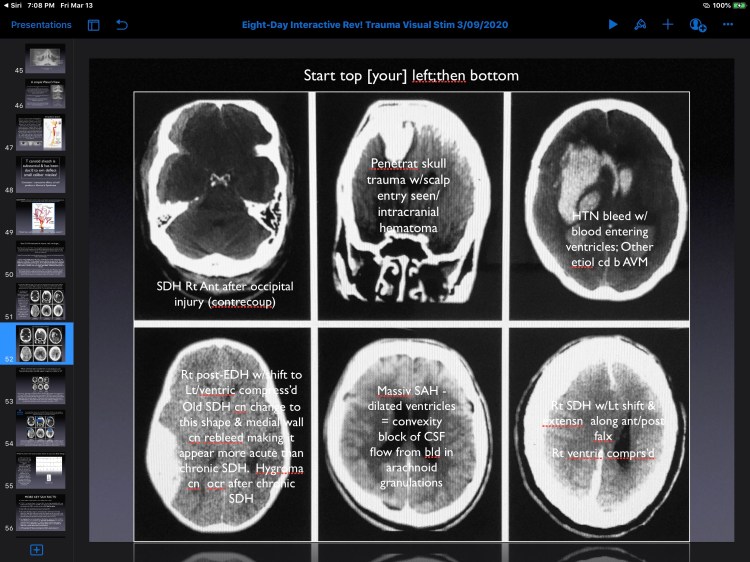
In this group the lower middle slice is of a patient who would likely arrive dead: he has a massive SAH that surrounds all of the cortical surfaces/even extends a long the falx in the midline [appears fuzzy due to blood filling the subarachnoid spaces immediately adjacent to the cortical sulci and gyri. The ventricles are dilated due to blood causing a CSF convexity block. So you can’t save him. The arachnoid granulations are all blocked…CSF can’t exit the head so the ICP is markedly elevated. In the midline [along the falx cerebrii] the blood appears fuzzy because it is a thin film that follows the sulci/gyri closely…it often looks like a zipper…described as the “zipper sign” and proves its a SAH along both sides of the falx. No intervention for this patient.
Next, the patient in the upper middle slice has a knife blade penetrating into the brain: traumatic penetration by knife [knife not visible on this slice] requires immediate transfer [1st] especially if no other injury. The knife should not be removed in the ED.
The upper left slice is of a patient with the lowest acuity [a right frontotemporal SDH [venous bleeding] and could be transferred last in this mass casualty simulation. However, this patient requires RSI before transfer. This patient has has midline extension and a collapsed ventricle [mass effect] which should improve w/measures to lower the ICP…treat and transfer simultaneously [urgently].
An acute epidural hematoma is due to arterial hemorrhage [lens-shape-lower left slice and generally more acute than a SDH]. The issue…if hemodynamically normal with reactive pupils [intubate/mild hyperventilation after RSI [all get RSI except the SAH…he is dead]. An EDH might even require an emergency burrhole if the patient decompensates in the ED.
Next, a patient with a hypertensive bleed [upper right slice] requires mild hypervent/transfer ASAP & might survive, but the prognosis is poor. Decades prior if there was intraventricular blood most had very low survival…this is a patient with a right-sided AVM that ruptured [comorbidity: chronic hypertension]. The danger is the BP…do not lower the BP because with chronic hypertension cerebral perfusion is reset to a higher range to maintain cerebral blood flow; it is best to gently do RSI and transfer; this patient actually survived [as did all but the patient with the massive SAH].
The six patients:
This would be a crazy [once in a lifetime] shift…and you always remember crazy! Super-emotional events cause new neuronal connections in long term memory in both the right and left hippocampus].
Clinical Emergency Physician
Prior Faculty for Midwestern University
EM Author/Educator/Medical Ilustrator
Expertise: EM Pathophysiology and physiology [both pediatric/adult]
Designer of a silicone membrane ECMO [extracorporeal membrane oxygenator]
By 2005 trained ⅓ of the world’s EPs for EM board certification
Trained Oral Examiners for a decade: the Board of Certification in Emergency Medicine [5000 original members...now the second largest EM group in the United States]; he was a compensated consultant for that and numerous other emergency medicine organizations.
All of Dr Collman’s presentations have been Co-sponsored AMA/ACEP category 1 CME ACCME accreditation through the AAPS, National and The Fl Chapter of ACEP and The Fl Medical Association since 1989.
Publisher of numerous EM manuals, and educational materials [all items were have copyrighted notices and have been sold by the ACEP Bookstore]; all authored by Dr Collman: 2 Vol program syllabus of thousands of Q/As and pathophysiology discussions of all chapters from eds 3-8 of “The Study Guide” [All chapters of the core content knowledge for completion of an emergency medicine residency]; teachs Resususcitation, CV Emergencies, Pulmonary Emergencies, The EKG lab [the 60 most important EKGs/management; Truama Emergencies, Pain Mgmt, Orthopedic Emergencies, Toxicology [Toxins and Antidotes, HEENT Emergies, Environmental Emergencies, Pediatric Emergencies [500 Q/As], HIV/AIDs-Infectious Diseases, Emergencies, Rhematologic Emergencies, Neurologic Emergencies, Acid-Base/ABG Presentation, Dermatological Emergencies, CT/POCUS [point of care ultrasound], Bariatric Emergencies, Endocrine Emergencies.
Dr Collman is endorsed by his programs participants [12,000+]
Examples: Dr James SULLIVAN MD DABEM; and others program participants described Dr Collman as a “National Treasure”
Dr Collman grandfathered into EM after completing a rotating Gen Surg Internship at UCLA School of Medicine [June 1981].
He accepted a directorship position at age 25, the contract to Illustrate “Emergency Management of Pediatric Trauma” [author:Thom Mayor MD FACEP] published by WB Saunders
Dr Collman provides strong intellectual support to his program attendees...many chose him to be their permanent career mentor and return annually to his live interactive conferences.
Dr Collman has designed computer-based programming to numerous organizations in ACLS algorithms [Univ of Pisstburgh]
He provides Interactive grand rounds as Case Simulations by invitation:
He designed an 8-h Visual Stimuli Presentation for Johns Hopkins Dept of EM [their board prep program;a second 8 hr presentation “The Genitourinary System-a Comprehensive 8-hour Review”; he teaches each program Johns Hopkins University.
He trained Examiners for the BCEM [AAPS] Atlanta GA: presented a combined certification review [both certification part I/orals] numerous time in Atlanta, Hawaii, Lake Tahoe, and Orlando, Fl 1991-1996.
He created their entire bard exam [part I and Oral Examination and a computer-operated Visual Examination [2 Versions] in 1996. This included 700 certification test items and 25 Oral Examination Live Test Simulations as well as trained their AAPS [BCEM Examiners twice a year for 10 years [throughout the 1990s]
Texts Authored Editor in Chief 4th-7th Ed of: “Pearls of Wisdom in Emergency Medicine [7 eds] and 35 Cds [33 are critical analysis of the 52 OBT Live CD set: audio recording made Live at Conference [cost $1515.00 (Oral Board Case studies)+ ASA/APAP toxicology CDs [each is 1 hour w/manual purchase price $65.00 for each + “CT Video: CT for the Emergency Physician”. Videotaped Live in Boca Raton, FL by Pear Productions
Publication Study Quote: “Dwight Collman MD DABEM DABFM Provides the most rigorous CME Education”...documented by EM News and EMRA [in 2002 ranked Dr Collman’s EM 8-Day Interactive Review! with the top 8 University or top ACEP chapter programs [an independent study they published for all of America’s Emergency Medicine Residents preparing for their board certification examinations.
2009 Jan Issue EM News Editor-in-chief ranked Dr Collman as the “premier educator for board preparation in the US”
Core Competencies:
Bedside Clinical Instructor all EM Medicine Clinical assessment/training EPs in all EM Procedures [over 90 procedures]
Core competency: illustrates human Anatomy as it pertains to EM/EM procedures [he does this Live and his clients request to keep his illustrations]
Dr Collman edited Emergency Management of Pediatric Trauma [while he illustrated this First-Ever Text devoted to Pediatric Trauma; he spent 2 years creating the illustrations for this text 1983-1985 and they were reproduced and resold by the publisher and appear in the Pediatric Trauma Capter of The Text: The Clinical Practice of Emergency Medicine” Ed 1., author Ann Lattimer-Harwood-Nuss [now Professor Emeritus, retired].
Completed a Fellowship in Gen Anesthesia: University of Utah School of Medicine
Awarded 5 specialty rotations [mentorship programs in medical school:ICU
President: Collman Institute Inc [a Fl S-Corp] 1994-2007 .
Clinical practice x ~40 Yrs
ABEM certification
Life Fellow Am Board of Forensic Examiners
Trains EPs in triage/emergency Pt care/documentation to mitigate litigation risk
Has been awarded teaching contracts from over 400 US Hospitals
Trains EPs from every branch of the US Military since 1989 -first group included the CO of the Portsmouth, Va Naval residency [Michael Gonzalez MD FACEP who officially made the Oral Board Tutorial! As mandatory education to graduate his residency program in 1989.
I am a “trainer-educator, author, medical Illustrator”.
I have treated college students at no cost since the 1990s
Additional skills/competencies: Documentation [chart review consultatnt], Test item Writer [wrote the entire certification partI/part II examinations in 1996
Teach/train using interactivity/I teach the statistical/mathematical precognitive approach to physicians for pediatric IV fluid protocols for resuscitation, 3 forms of dehydration, burn fluid calculations + formula for airway [pulmonary burns] 52 simulations in 5 days; the role of the CANs/EXRs; I have a program syllabus for both of my CME programs
Program author/presenter: “The Clinical Documentation Of the Emergency Medicine Hospital Chart”, a 2-Day program conducted in Park City, Utah [1992]
As a Forensic Examiner he has reviewed and consulted emergency Physician defendants [approx 30 cases over 25 years]
View more posts